Here’s a bit of an odd-and-ends post covering some common questions I’ve been getting about COVID-19 and infection control in veterinary clinics. As always, answers are based on little or no evidence, but on principles of infection control, and they may change as we learn more and as this pandemic continues to evolve.
Would it be safe to let one client per pet into our building, if they have to wear a mask and use hand sanitizer on entry? And only letting a client in that has to see a veterinarian. Not to buy merchandise.
“Safe” is subjective and a moving target. Realistically, we’re looking at gradations of risk. There’s always some, and the closer and more prolonged the contact, the greater the risk. Having a client in the clinic is riskier than having them outside, undoubtedly. If they come into the clinic, the measures described (especially mask use) can help minimize that risk. There’s no way to say how much risk is present because we still have limited data, and where you are would be a major factor, based on the local epidemiology of the virus (which also changes). In some places, community disease activity is very low, so the odds of any single person who comes into your clinic being infected are exceptionally low. That’s not true everywhere, though.
Ultimately, our goal is to keep people out of clinics as the default. If there’s a solid reason for them to come in, then the risk goes up, but that can be mitigated through minimizing the closeness and duration of contact, wearing masks and good hygiene. It comes down to the cost-benefit… how important it is for the client to be in the building vs the risk you (and all the staff) are willing to take (and the ability to make sure preventive measures get done).
That’s a bit of a non-answer but there isn’t really a yes/no response to a question like that, unfortunately.
Some people recommend to use a coffee filter or towel sheet with reusable masks. What do you think about that and if it’s a good idea, is it okay to use in surgery and how many hours does it last?
For surgery, I’d rather use a proper surgical mask, if you have access to them. Their performance is more predictable, and surgery is a higher risk environment. If you’re low on surgical masks, then a cloth mask is a tolerable backup (although I’d be a bit wary of using a cloth mask for a surgical procedure involving an implant). I haven’t seen anything that indicates those extra filters in masks do much. I assume they don’t make anything worse (unless they make it harder to breathe or are so resistant to airflow that they direct more unfiltered air out the sides of the mask), but I don’t recommend them over regular cloth masks.
What should we do about dental procedures on small animals? (I’ve had dozens of variations of this question.)
Cat dentals are the big question, and a lot of the uncertainly relates to a lack of understanding of the prevalence of SARS-CoV-2 in cats, particularly cats from households that are not flagged as high-risk based on querying the owner’s health status. Risk also varies geographically, since the risk from cats directly parallels the risk of people being infected in the same region. In many areas, the odds of a cat from a purportedly healthy household being infected are probably exceptionally low. However, we don’t have enough data to say much more, and as disease activity varies, the risk will vary. We’re trying to answer some of those questions with PCR-based surveillance as well as an upcoming seroprevalence study. In the interim, there’s a realistic “life has to go on” component, since we will be dealing with this virus for a long time.
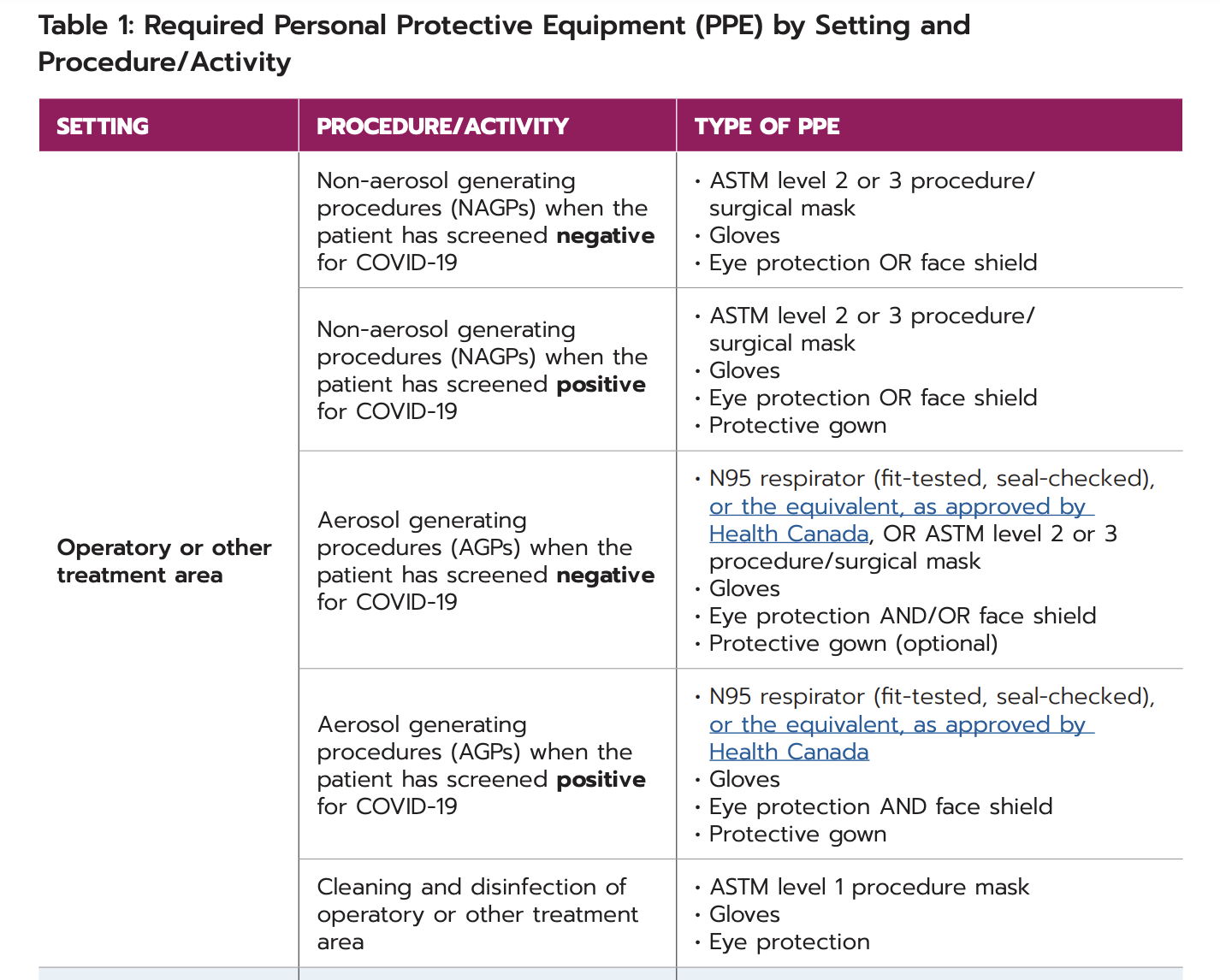
For now, a key step is screening the owners for current or recent respiratory disease. It’s not a guarantee, but restricting these procedures to pets from healthy owners should help drop the risk a lot. Beyond that, it’s mainly PPE. Aerosol generation is an inherent issue with dentistry, but exposure can still be minimized with appropriate PPE, cleaning and disinfection and other basic infection control practices. I think we can look to human dentistry here, since they are dealing with even greater risks. Below is a table from an Ontario guidelines document. In this table, “positive” and “negative” refer to syndromic screening, the same as we would do for owners of animals coming to a veterinary clinic. They recommend N95 respirators for aerosol generating procedures (AGPs), regardless of screening status, presumably based on the risk of asymptomatic shedding in the general population. However, they give the option of surgical masks for lower risk patients and procedures. Our risk as veterinarians is presumably lower than theirs, so the decision of whether to wear an N95 plus eye protection vs a surgical mask plus eye protection may come down to mask availability, understanding of COVID-19 activity in the area, and risk aversion. The key is to wear A mask of some kind, and to wear eye protection as well (the latter in particular is not consistently done in veterinary medicine).
If N95 masks are used, they would only be required for those in close proximity to the AGP. It’s debatable whether technicians and anethesiologists would need this level of protection (vs a surgical mask), especially when surgical masks are considered tolerable for AGPs in low-risk human patients. People coming in and out of the dental suite (which should be minimized in any case), or who are farther from the patient’s mouth would be much lower risk for exposure.
Cleaning and disinfection of areas potentially contaminated by aerosols is also important. People generally do a good job on disinfecting tables and countertops, but don’t think about the other areas or surfaces that get contaminated by aerosols, like the anesthetic machine for example. That also highlights the need for a good OR/dental suite environment with limited open storage. We don’t want aerosols contaminating things that people will use for subsequent procedures (e.g. gauze sponges, suture packs), so if an AGP is being performed, it’s best to make sure that the area is as barren as possible.
With some basic practices like that, the risk of SARS-CoV-2 transmission related to doing a cat dental is probably much greater from the transfer of the animal to/from the owner, than from the cat during the procedure itself. That’s why we need to focus on physical distancing from owners as much as possible.