Here’s a break from COVID-19 posts, because other infectious disease challenges do still exist!
The latest edition of Emerging Infectious Diseases has an interesting paper that provides an overview of a decade’s worth of cases of the fungal disease blastomycosis in Minnesota. Blastomycosis is caused by the fungus Blastomyces dermatitidis. It’s called a “dimorphic” fungus because it lives in two forms. In the environment it lives in the form of a mold, and it’s exposure to this form that can result in infection in people and animals. Once it finds its way into the body, it changes to a yeast form, which then grows and causes disease. People and dogs get infected the same way, from environmental exposure. While infected dogs and people don’t pass on the fungus to other individuals (animal or human), knowing about infections in one species can inform us about risk in the other in the same area.
The paper (Ireland et al. 2020) summarizes all the reported human cases of blastomycosis in Minnesota from 1999-2018. This disease is reportable in the state, so when it’s diagnosed in a person, there’s a requirement to notify the health authorities. The authors collected information about the cases and asked as many patients as they could about various types of exposures in the preceding 3 months. Here are some of the highlights of their results:
- There were 671 confirmed cases during the period, with a range of 22-58 per year.
- 32 case were part of outbreaks, including one outbreak where people and dogs got sick from excavation for a new housing development.
- 69% of people were hospitalized, with the duration of hospitalization ranging from 1-197 days (median 8 days).
- Most infections (72%) were respiratory tract infections, 21% were disseminated (infection of several body sites) and 7% were local infections at sites other than the lungs.
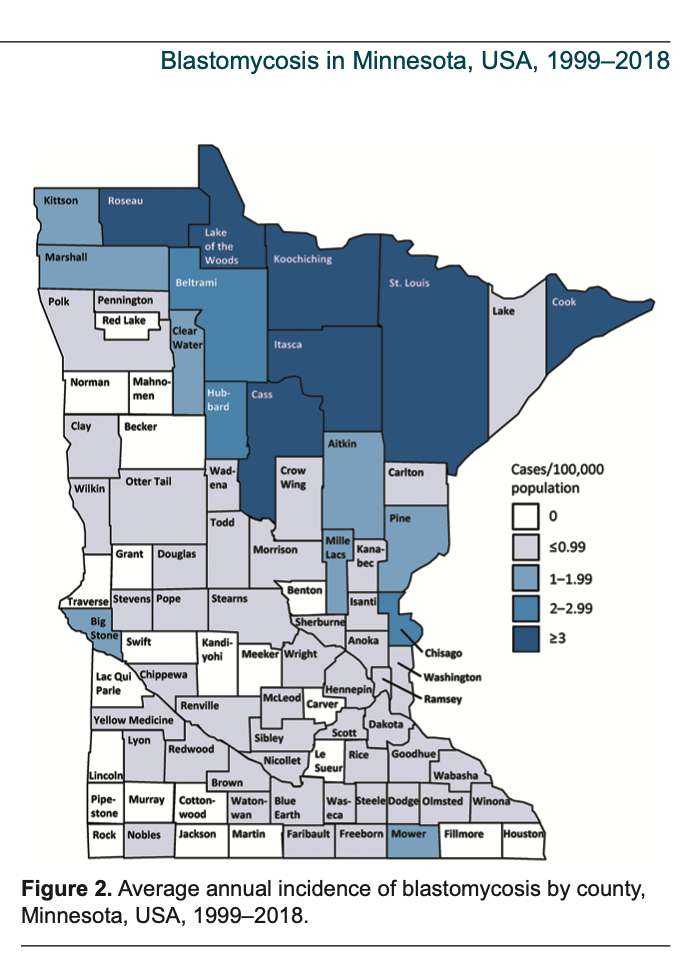
- Infections were not evenly distributed across the state. Northern areas were more heavily impacted (see figure below).
- Prompt diagnosis is often a challenge with this infection – 27% of people went more than 30 days before being diagnosed, and 67% of the time, a diagnosis wasn’t made until the time of hospitalization.
- Overall, 10% of cases died.
Getting to the dog-related aspects, 53% of people with blastomycosis had a dog, and 10% had a dog that had previously had blastomycosis (4% had a family member that had previously been infected). That’s not a huge percentage, but it’s important to consider alongside the information above about the time delay to diagnosis. Knowing about the disease in the dog may help speed up diagnosis in a person.
That said, if you have a dog that develops blastomycosis, you shouldn’t panic or rush to your physician if you are healthy. However, it’s information to store in your brain and to tell your healthcare provider if you do get sick, particularly with unknown lung disease. Most of the time it won’t be blasto, but it costs nothing and takes a few seconds to tell your doctor about your dog. It’s particularly important for people who visit higher risk areas but live in lower risk areas. Around here, some common summer vacation home areas are high risk, but the risks are very low in urban centres not far away. So, blasto might not be top of mind for a physician if they don’t know about the travel/vacation risk.
We don’t have a formal blastomycosis surveillance program to help link up human and canine disease in Ontario. We tried a few years ago and trying again has been on my to-do list, but there are some logistical challenges. While we’re still hoping for better surveillance, a little awareness can go a long way.