Words matter.
Inconsistency and inaccuracy with terminology can result in misinterpretation, poor communication and create challenges when discussing cases, interpreting research and developing guidelines.
This has been quite evident with urinary tract disease in dogs and cats. For example “urinary tract infection” is a very commonly used but very generic term. It has been used for bacterial cystitis, subclinical bacteriuria, a positive urine culture, positive urine cytology, pyelonephritis or a few other conditions, or, often, indistinct combinations of those. This creates a lot of challenges since those are vastly different issues, and when we’re not speaking the same language or when we’re mixing completely different diseases into the same bundle, we create the potential for error, misdirection and misunderstanding.
So, we decided to do something about it, as part of our ongoing revision of the International Society for Companion Animal Infectious Diseases (ISCAID) urinary treatment guidelines.
The guideline field has advanced a lot in recent years, for the good. We’re getting past the time where you could just get a few smart people in a room and come up with a guideline. Those were often quite good and they were really important stepping stones. However, lack of broad representation, involvement of stakeholders, consideration of biases and other issues were limitations. The same applies for setting definitions. While it would be easy to get a group of people together to make definitions, we need to be more rigourous.
As a result, we started an initiative to develop consensus-based definitions using a broad group of international participants. That consisted of a steering committee to start things off (5 people from 4 countries), ISCAID guideline working group member review (19 people) and then two broader rounds of input from 90 people from 19 countries. All the methodological details are in the paper (Weese et al 2026) for anyone that wants to see it, but the goal was to engage a broad range of people with expertise, going through multiple rounds of review and suggestions to arrive at consensus.
We tried to be as transparent as possible, explaining what was done each round, why decisions were made and showing some terms/definitions that we abandoned (and why). It wasn’t necessarily easy, but I think it ended up yielding some solid results, with a lot of good discussion along the way.
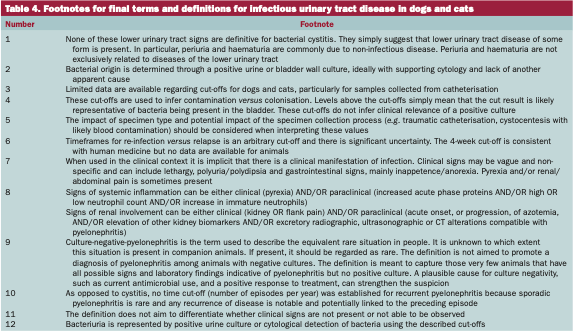
I won’t go over all the results since there’s a lot of information. The final definitions and associated footnote are in the images below. For more context (and maybe easier reading), the paper is open access.

Are these perfect? Probably not. Did we include everyone that might have had useful input? Definitely not. However, they’re a step along the way.
As we said in the paper’s conclusions, “Standardisation of terminology is a foundational component of clinical communication, clinical research, surveillance and guideline development. This initiative has allowed for the creation of terms and definitions based on broad stakeholder consensus. The study’s output should assist with ongoing and future efforts to improve the evidence base pertaining to infectious urinary tract disease and foster improved clinical guidance.”