Canine heartworm (Dirofilara immitis) is a nasty parasitic infection of dogs that’s relatively rare in Canada, but it’s still a concern because of how severe it can be and because treatment isn’t easy. It’s transmitted by mosquitos (we have lots of those), but transmission is also influenced by temperature (which varies a lot in Canada over the year).
Heartworm control focuses on regular administration of preventive medications that are typically given to dogs monthly, either during the heartworm transmission season or all year round. The medication is often combined with flea/tick preventives and/or other antiparasitics.
We have a seasonal risk period for heartworm in Canada, and it’s pretty short in some areas. We want to maximize use of heartworm preventive drugs during that period, so understanding exactly when the risk is present is important. Since transmission is temperature-dependent, the transmission period will vary across the country, and as out climate changes over the years, we need to keep re-evaluating the timing for giving dogs preventatives.
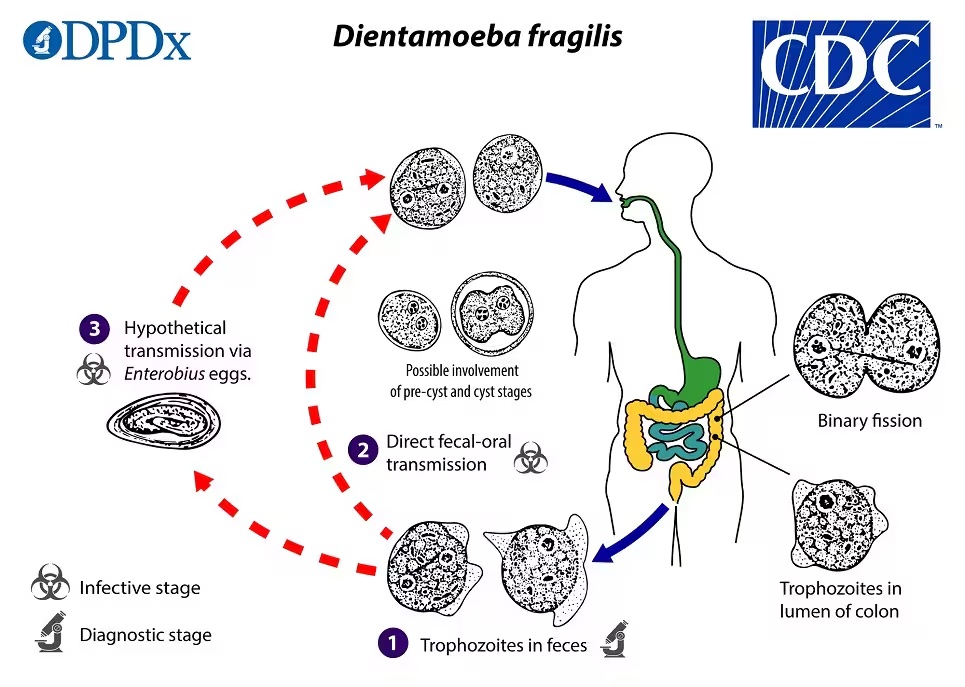
Reminder: Heartworm life cycle
Canids (including dogs and wild canids, like coyotes) are the reservoirs for this parasite . Adult heartworms produce microfilaria which are found in the dog’s bloodstream. These are picked up by mosquitoes when they feed on a dog. They then develop into the mosquito from microfilaria to L1, L2 and then L3 larvae (L3s are the infectious form). At that point, if the mosquito bites another dog, it can transmit heartworm via the L3 larvae.
Why is temperature important?
Heartworm larval maturation stops at temperatures less than 14C (57F), so the time that it takes for an infected mosquito to be able to transmit infectious heartworm larvae depends on the time that’s above 14C, and how far above 14C the temperature is. We measure this in “heartworm development units” (HDUs), which are calculated by taking the mean (not maximum) daily temperature in Celcius and subtracting 14. If it’s a positive number, that’s the number of HDUs for that day.
Today, the mean temperature will be around 0C here. So, if there was an infected mosquito, the heartworm larvae are not developing. Hopefully things will warm up soon. If we get a day when the mean temperature is 17C, then we’ve accumulated 3 HDUs for that day. Once we get a total of 130 HDUs, those larvae should be infectious. That obviously takes time in spring in Canada, but not much time in places like the southern US when mean daily temperature is consistently and substantially higher, and 130 HDUs can be accumulated quickly, any time of the year.
In Canada, June 1 has traditionally been the recommended starting date for heartworm prevention. That was based on temperature data from Windsor, Ontario (pretty much as far south as you can get in Canada) plus a very safe buffer period. However, since data for this recommendation were from 1957-1986, we figured it was worth rechecking, and we published the results in December in the Canadian Veterinary Journal (CVJ)(Weese & Peregrine, 2024).
The short answer: our current approach is still good.
We looked at temperature data from 1996-2023 for a variety of cities in Ontario, and how long it took for 130 HDUs to be accumulated. (I’ve put together data for cities in other provinces too but haven’t done anything with those yet.) The results are shown in the table below. In southern Ontario, the risk typically started mid June. In Windsor, it was as early as May 25, but with a median of June 7. Some years, the risk started quite late, and in some northern cities it didn’t start until August.

Okay, but May 25 is before June 1, so is it a problem to still use that date as the start of the risk period, at least in Windsor?
- No. Fortunately, our heartworm preventive drugs will kill L3 and early L4 stages, so they will kill larvae up to 4 weeks after infection. If a dog was infected May 25, preventive administration as late as June 22 would still work.
If we want to look at the limits for when we should start preventive treatment, it’s actually the date that 130 HDUs are accumulated plus 28 days. I definitely wouldn’t want to cut it too close, and since we don’t track HDU accumulation in real time (and there are some potential disclaimers), we want to give ourselves a good cushion in terms of timing.
What about climate change?
Climate change is real, but mean temperature changes are slow and gradual. The graph below shows the trends over time. In some locations, there was a significant trend towards earlier dates of 130 HDU accumulation. In others, there was actually a trend towards later. Overall, there was no significant change. However, it’s fair to expect that there will be gradual changes over time, so we’ll just need to keep checking in.

Can we trust the 130 HDU requirement?
Mother Nature’s always a bit unpredictable, but the 130 HDU threshold has been validated pretty well. Even if the threshold was lowered to something like 125 HDUs, it would only change the typical time to accumulation by one or two days.
When we’re assessing risk periods, we want to err on the side of over-estimating, not under-estimating risk, so we took a conservative approach with our methods. You can calculate HDU accumulation two ways: 1) simply calculating the time until 130 HDUs is hit in the spring, or 2) using a 30 day rolling window. The latter is based on an assumption that adult mosquitoes only live for a maximum of 30 days, so early warm periods become irrelevant if the mosquito dies before larvae can become infectious. We chose to use the total time, not the 30 day window, since there is evidence that some mosquitoes can live for over 30 days.
There are also potential issues such as microclimates (mosquitoes living in a warmer local site like a building or sewer) and heat sinks. Whether this is relevant to heartworm transmission is unclear, but it’s probably a minor issue, if it’s an issue at all.
What does this mean for routine heartworm prevention?
It means that it’s still fine to use June 1 as the start of the risk period in Canada, even in extreme southwestern Ontario. We don’t need to worry about starting earlier (a question I get all the time), at least not yet. June 1 still provides a good cushion too, for situations where people are late getting or starting the prescribed drug.
But… don’t forget about ticks!
Ticks are different. The tick risk season is much longer than the heartworm risk season. We have some risk of tick activity anytime the temperature is above 4C (or maybe even lower). Obviously, that means we have risk of tick exposure well before risk of heartworm exposure, and we have problems with people starting tick prevention too late because they only think about the June 1 heartworm risk date. If ticks are a concern, then tick prevention earlier in the year is important (and if it’s combined with heartworm preventive, the heartworm start date discussion becomes a moot point).